James M. Swinehart, M.D. |
Liposuction previously performed under general anesthesia is now a little-utilized approach. This method was responsible not only for initially negative public attitude, but also for considerable morbidity and mortality with pain, bleeding, bruising, and prolonged recovery times. |
| Now, however, the only similarity of tumescent liposuction to the "old method" is that fat is removed from the body through a tube. Several important modifications of the operative technique have greatly refined liposculpture into an art form. These developments include the use of tiny incisions (which disappear without suturing), special post operative dressings and garments, efficient pumps for local anesthesia infusion and liposuction, and precisely engineered microcannulas designed for each body area and special situations. We will now examine treatment of specific body areas in men and women. |
44 year old white female with good skin tone, but with excess abdominal, midriff, and flank fat. |
Note uniform, even contraction of skin with undetectable result. |
Obese 66 year old female patient with striae (stretch marks), abdominal panniculus, and loose skin tone. |
Result 3 ½ weeks later. Although striae remain, skin has retracted well and patient was happy with result. |
| Some body areas and some patient types, are, of course, more prone to asymmetry than others. A 22 year old athletic single female with excellent skin tone will show little or no evidence of surgery (other than a nicer contour) two weeks after the procedure. On the other hand, a patient who is overweight, flabby, who has not exercised in years, and has had children, should never expect close to a perfect result. Abdominal asymmetry is particularly likely in female patients, especially those with surgical scars and the above-mentioned conditions, whereas, male patients seem to show little or no irregularity. The midriff and waist areas are more fibrous in nature. Asymmetry is uncommon here, except where the flank liposuction is feathered onto the back. |
"Angel wings" on back causing unwanted bulges when patient's bra was fastened. |
Flattening and disappearance after targeted liposculpture. |
| Many men are self-conscious of the fat on their chest (male breast). Significant improvement can be obtained via two crisscrossed incisions — one in the inframammary area and one in the axilla. |
Male patient in excellent physical condition but with unwanted breast fat. |
Flattening to nice athletic contour with tumescent liposculpture. |
| Tumescent liposuction of the buttocks can be a difficult maneuver. Preexisting cellulite and uneven skin folds can be a significant hindrance to an even outcome. The dermatologic surgeon must be careful not to remove too much fat, and to perform most of the fat removal in a superior direction from an incision in the intergluteal crease in the prone position, comparing both buttocks when finished. The soft, easily removed fat present on the inner thighs makes over-correction a real risk. One must proceed slowly and evenly, using very fine cannulas (12 gauge or smaller). It is very important to crisscross the tunnels through anterior and posterior incisions. Klein and Cook have each developed foam pillows to elevate the opposite flexed knee, placing the inner thigh on a horizontal plane accessible from a posterior incision. One generally starts with a 12 and/or 14 gauge cannula to set the tunnels, followed by a 3mm cannula, followed by a 12 or 14 gauge cannula gauge for fine feathering. |
Prominent excess fat on inner thighs, as well as abdomen and hips. |
Remarkable improvement in all areas with even, symmetrical results seen only three weeks later. |
| Likewise, asymmetry is common in the saddlebag areas. This may be due to the fact that the pinch technique is difficult to employ here, or that variation or position can alter the intraoperative appearance and direction of the tunnels. It is common to leave too much fat in the posterior saddle bag near the buttock, whereas one must be careful to avoid the trochanteric depression. Feathering should be carried down onto the lateral thigh. The results obtained, however, are gratifying to many patients. |
Unwanted bulges on saddle bags (lateral thighs), as well as hips, inner thighs, and knees. |
Beautiful results seen in all areas treated. Note also the improvement in patient's skin tone. |
| Lipsuction of the knees often yields beautiful results, but feathering must be skillfully blended into non-suctioned areas of the middle third of the inner thigh. Liposuction of the upper arms must be blended onto the infrascapular and infraclavicular areas to avoid an uneven appearance. The skin nearly always retracts in this location in relatively young patients with good skin tone. |
Unwanted knee fat pads give the patient a bow legged appearance. The dermatologic surgeon should avoid treating the middle third of the thigh while removing fat from the inner thigh and knee regions. |
Uniform, even outcome after liposculpture. Note that the objective of a straight line from the inner thigh to the knee has been achieved giving the patient a much thinner appearance. |
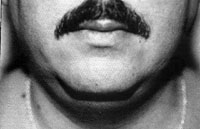
Female patient with fat accumulation in chin and neck. |
Note complete retraction of skin following this procedure. |
| Many patients request liposculpture of the face, neck, chin, and jowls. Indeed, some patients wish body contouring to be performed only in this region. Asymmetry is uncommon with neck liposuction, where the surgeon strives to remove essentially all of the fat. However, considerable surgical skill is needed to avoid a "hollow" appearance following liposuction of the cheeks. Although the procedure is not a substitute for a facelift, a considerable amount of fat can be removed, with significant correction, of the jowls and neck. Because of the fact that hundreds of tiny tunnels are created (rather than one large cavity), this skin nearly always completely retracts to a pleasing contour. |
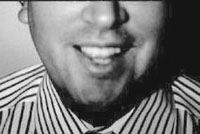
This 30 year old patient, although thin, was often judged to be overweight because of his double chin. |
After liposculpture, his neck contour matches the rest of his thin body. |
Same patient, lateral view, showing large fat pads external to platysma muscle. |
Note complete retraction of skin with smooth aesthetic contour. |
CORRECTION OF ASYMMETRY Rather than having to correct asymmetry, it is hoped that the dermatologic surgeon can prevent this outcome by utilizing the principles listed herein. However, in patients with preexisting deformities, patients who have had previous liposuction, or in patients with predisposing conditions such as sun damage or poor skin tone, the physician must be able to address this problem. |
Female patient before liposuction |
After liposuction revealing depression in thigh |
Area to be treated with fat injection is marked and anesthetized |
Beautiful correction from fat transplantation |
FAT TRANSPLANTATION Fat transplantation is often quite successful for correction of post liposuction depressions. The donor fat can, of course, be removed from another area where too little fat was removed initially. Should such an area not exist, the author prefers the upper outer quadrant of the buttock as a donor source. Many methods exist for lipoinjection, and controversy exists presently over the role of washing and centrifugation. One should, however, develop a personal technique whereby living fat cells can be injected to achieve slight over-correction soon as their removal from the donor area. Dermal grafting, as described by Dr. Swinehart in the American Journal of Cosmetic Surgery, may also show future promise for correction of soft tissue defects. |
Cellulite release tool |
"Cellulite" depressions on lateral thigh |
Improvement noted after cellulite release technique |
TREATMENT OF CELLULITE We've probably all seen, or experienced, those cottage-cheese like dimples or ripples on the hips or thighs known as "cellulite." Purported treatments for these are likely as old as mankind — but do they really work? First, a word about its origin. Cellulite may be present at an early age. The author can visualize dimpling on his six year old son's backside in the right light! Medically, this condition seems to be like the tufting on a sofa; fibrous bands pull certain areas of the skin downward into small depressions, or pits. Another theory centers on decreased circulation of the skin, leading to protein deposits and irregular fat lobules. Weight gain, of course, contributes to the problem. In years past, salons and therapists have employed electric current, as well as vibrating massage belts, to reduce fat and cellulite. Additionally, heat, herbal packs, and "exothermic massage" have been tried. More recently, attention has focused on the use of Xanthines (caffeine, theophylline, aminophylline) for treatment of cellulite. The true effect of these therapies is unknown. Since thigh diameter and water content varies not only with the time of day but also with factors such as menstruation, small changes in measurements should not be used to substantiate these claims. Tumescent liposuction, while effective in removing fat, may or may not improve this dimpled condition. Vigorous exercise, by enlarging the underlying muscles, can often produce improvement. Finally, the new "cellulite release" technique also holds promise in some conditions. |
Athletic female patient who could not lose fat from saddle bags, inner thighs, or knees even with vigorous exercise and dieting. |
One photo says it all — this patient has gone from an "8" to a "10" with tumescent liposculpture by Dr. Swinehart. |
ULTRASONIC LIPOSUCTION An Italian surgeon, Zocchi, has researched the use of ultrasound in fat transplantation and liposuction for the past 10 years. He has proposed a technique whereby ultrasound is first applied to heat, liquefy and soften the targeted fat pads. Following this maneuver, the liquid fat is removed by suction in the usual fashion. The concept is, however, still under investigation and possesses certain limitations. For one thing, the tumescent technique, with its high pressure infusion pumps produces sufficient tissue turgor to facilitate rapid dissolution and removal of the tumesced fat. Also, the application of hard to control heat induces the risk that thermal trauma may damage fat tissues in an uneven fashion, thus inducing surface irregularities and post inflammatory hyperpigmentation. The use of ultrasound adds more time to a finesse procedure that already takes two to three hours. Finally, as noted by Jeff Klein, the California dermatologic surgeon who originated tumescent liposuction — why add complexity to a procedure that is refined, predictable, and nearly always produces aesthetically pleasing results? This technique needs further development and study before being released for widespread public use. In summary, tumescent liposculpture has revolutionized the field of body contouring by providing a means of safe, efficient, bloodless fat removal under local anesthesia. Newer instrumentation has given the dermatologic surgeon the tools to achieve outstanding results in selected instances. Attention to the surgical maneuvers described above will, hopefully, enable the liposculpture specialist to perfect, with finesse, the anticipated surgical outcomes to an even high degree. Dr. Swinehart specializes in Tumescent Liposculpture at 950 E. Harvard Avenue, #630, Denver, CO 80210 - Phone (303) 744-1202. Copyright 1997 CDC. |